
Receipts: Universal Healthcare Costs Less and Performs Better

More than 70 countries, including all of America’s peer nations, have universal healthcare, but the United States does not. When the discussion about switching to universal healthcare is brought up, we’re told it would cost too much, increase wait times, and worsen outcomes. The reality is the opposite.
Our peer nations have lower costs, better broad health outcomes, higher rates of insurance coverage, and often better access to routine, preventive, and time-sensitive care.
Universal healthcare is the better approach, and there are many ways to implement it, including single-payer, multipayer, and public-private partnerships.
Let’s look at the facts and clear up the misinformation.
Universal Healthcare Costs Less
The first argument made against universal healthcare is that it would cost too much to implement. That is not true.
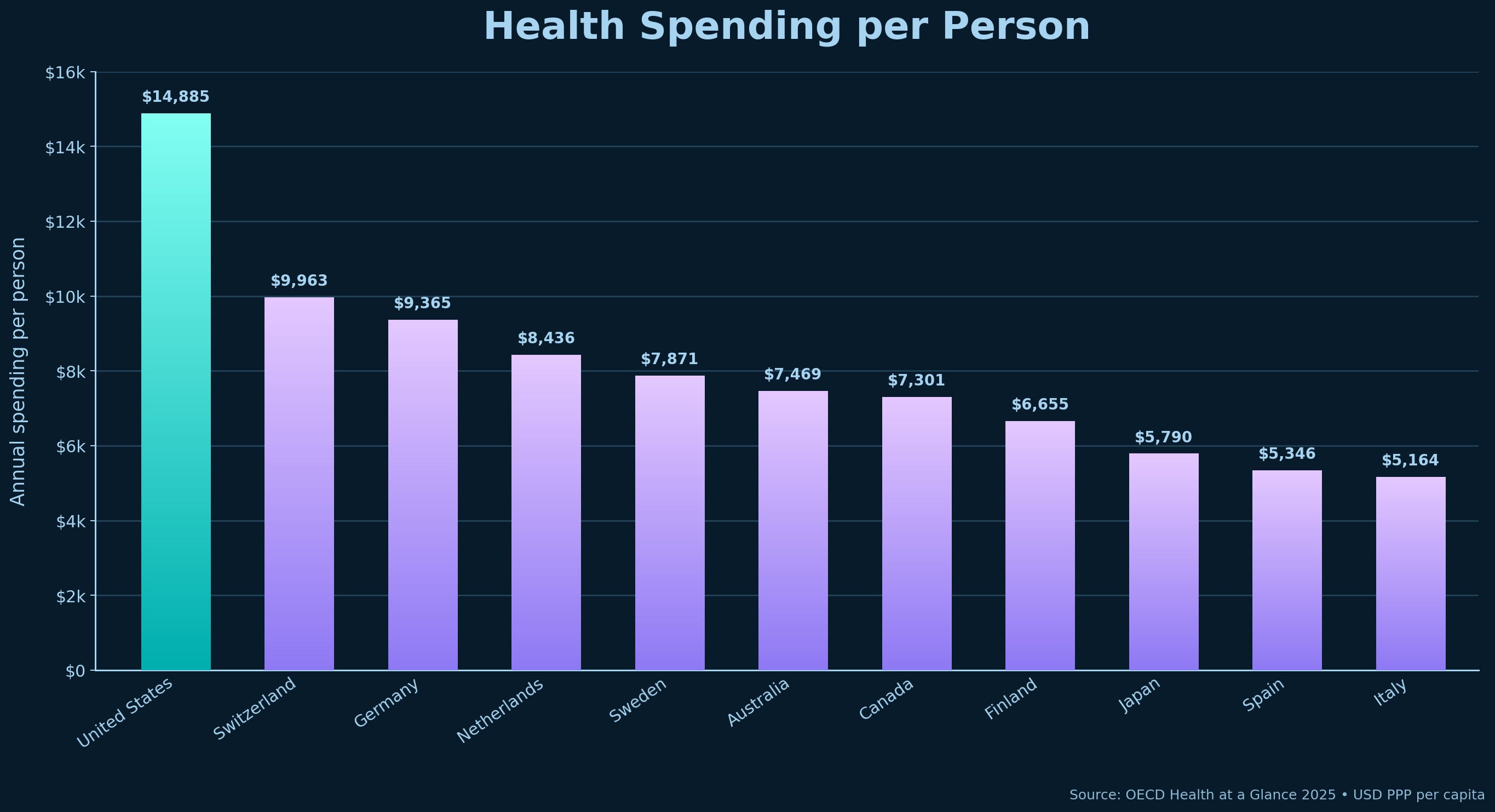
America currently spends more on healthcare than any other nation, and by a wide margin. The United States spends almost $15,000 per person on healthcare. Germany spends around $9,400. Japan spends about $5,800.
We can see differences in spending by looking at the costs of medical care across countries. The following numbers are median claims costs, meaning the cost going through the healthcare system, not necessarily the exact out-of-pocket cost paid directly by the patient.
One syringe of Ozempic costs $861 in the US. In Spain, it is $140. In Germany, $85.
40mg of Humira costs Americans over $6,000. In Spain, that is under $1,200. In Germany, it is $1,043.
4 syringes of Enbrel also cost over $6,000 in America. In Spain, that costs ~$800. In Germany, ~$1,000
The costs of procedures in the US are also high.
Coronary bypass surgery will cost you $89,000 in America. In Germany, that is about $17,000. In Australia, $17,700.
A total hip replacement costs $29,000 in the US. In Australia, it costs $15,000. In Spain, $6,800.
An appendectomy will cost you $13,500 in the United States. In Australia, it costs $4,200. In Spain, only $2,600.
When someone asks how America could afford universal healthcare, the answer is that we are already paying more than any other nation. The real question is why we spend so much and still leave people uninsured, underinsured, buried in medical debt, or unable to afford the care they need. It isn’t about whether America can afford universal healthcare. It is that we cannot afford the system we currently have.
Switching to universal healthcare could save the country hundreds of billions of dollars each year, depending on the program implemented. PLOS Medicine reviewed an economic analysis of 22 single-payer healthcare plans and found that 19 would result in savings in the first year of implementation.
The savings come from reducing administrative waste, negotiating drug prices, controlling provider prices, and removing the expensive maze of private insurance billing.
Sources for this section
OECD Health at a Glance 2025: U.S. spending per person, GDP spending, and international comparisons
KFF/Peterson Health System Tracker: U.S. health spending compared with peer nations
PLOS Medicine review of single-payer financing studies
Universal Healthcare Improves Outcomes
Despite the United States’ excessive healthcare spending, it does not lead in a single health outcome and is far behind in many of the most important ones.
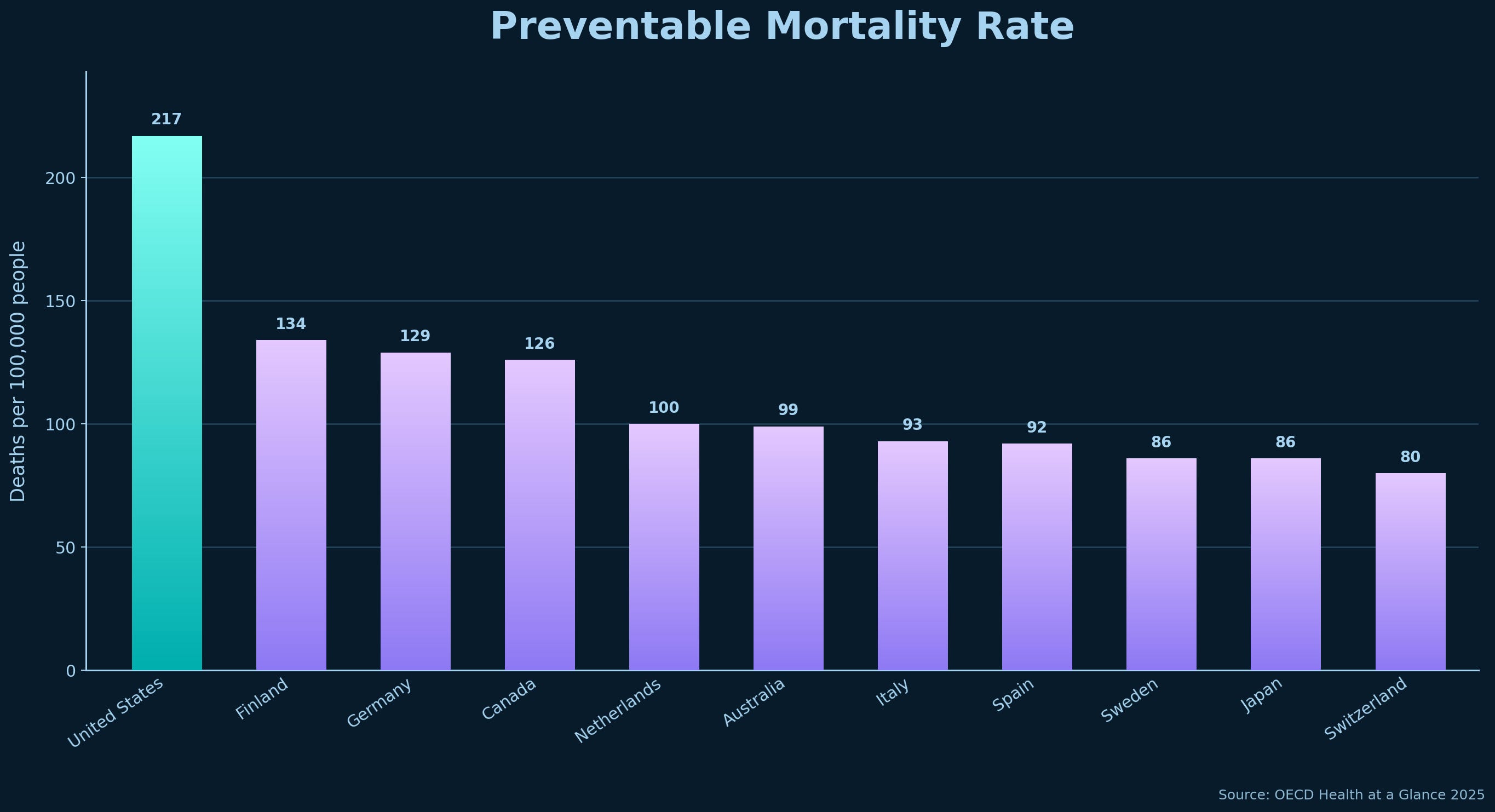
One of the most common metrics used to evaluate healthcare is preventable mortality. These are deaths that could have been prevented through public health and safety measures and effective early intervention. The United States has 217 preventable deaths per 100,000 people. Australia has 99. Japan has 86. They both spend far less per person for healthcare.
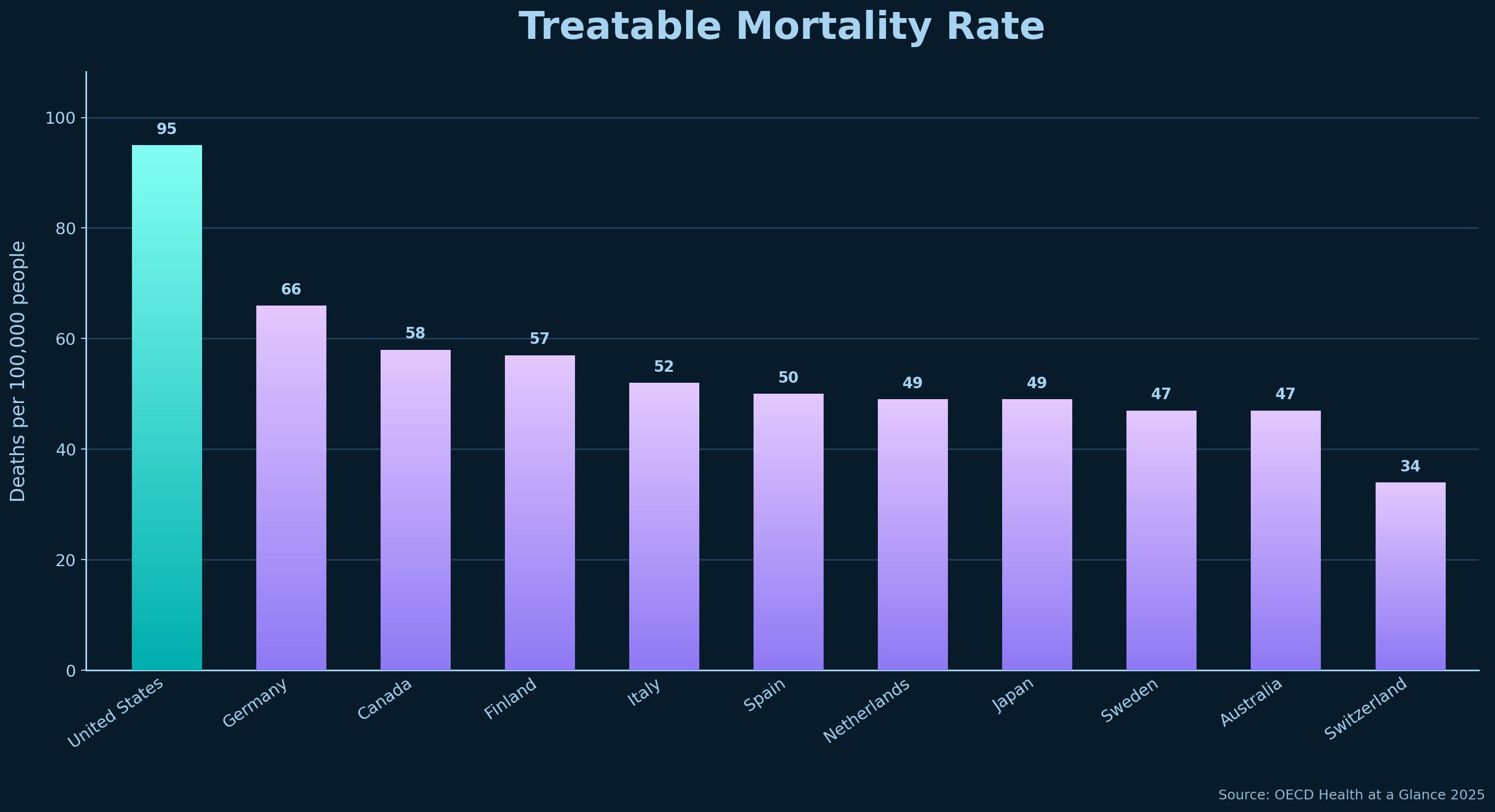
Another version of that evaluation is treatable mortality. The difference is that treatable mortality looks at deaths that could have been avoided through timely and effective medical care after a condition develops. Again, we see the United States with a high number of 95 per 100,000 people, compared to Australia’s 47 and Japan’s 49.
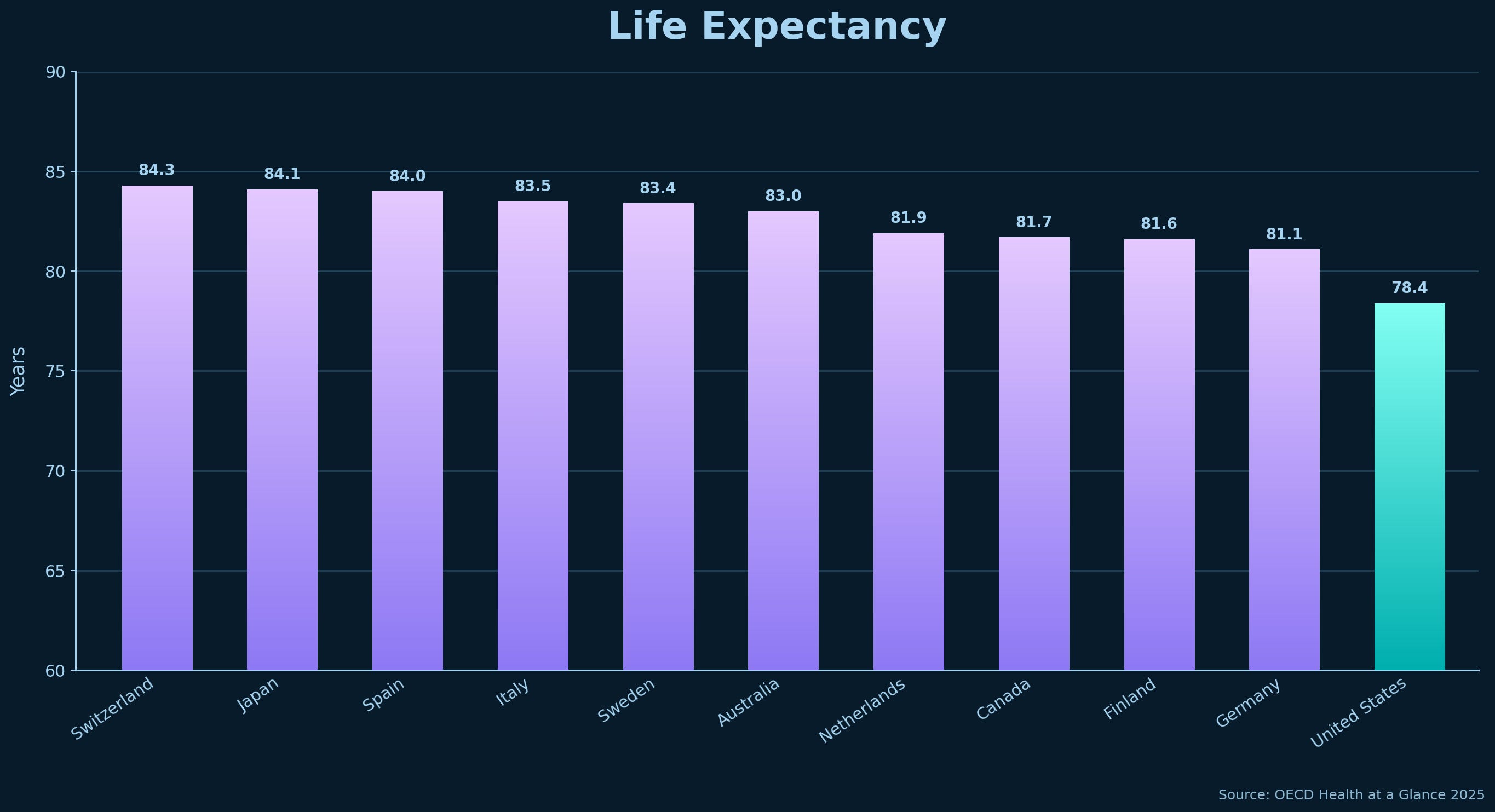
Then there is life expectancy, which is simply the average number of years a person is expected to live. The United States has a paltry life expectancy of 78.4 years. Australia is 83 years, and Japan remains near the top of the charts at 84.1 years.
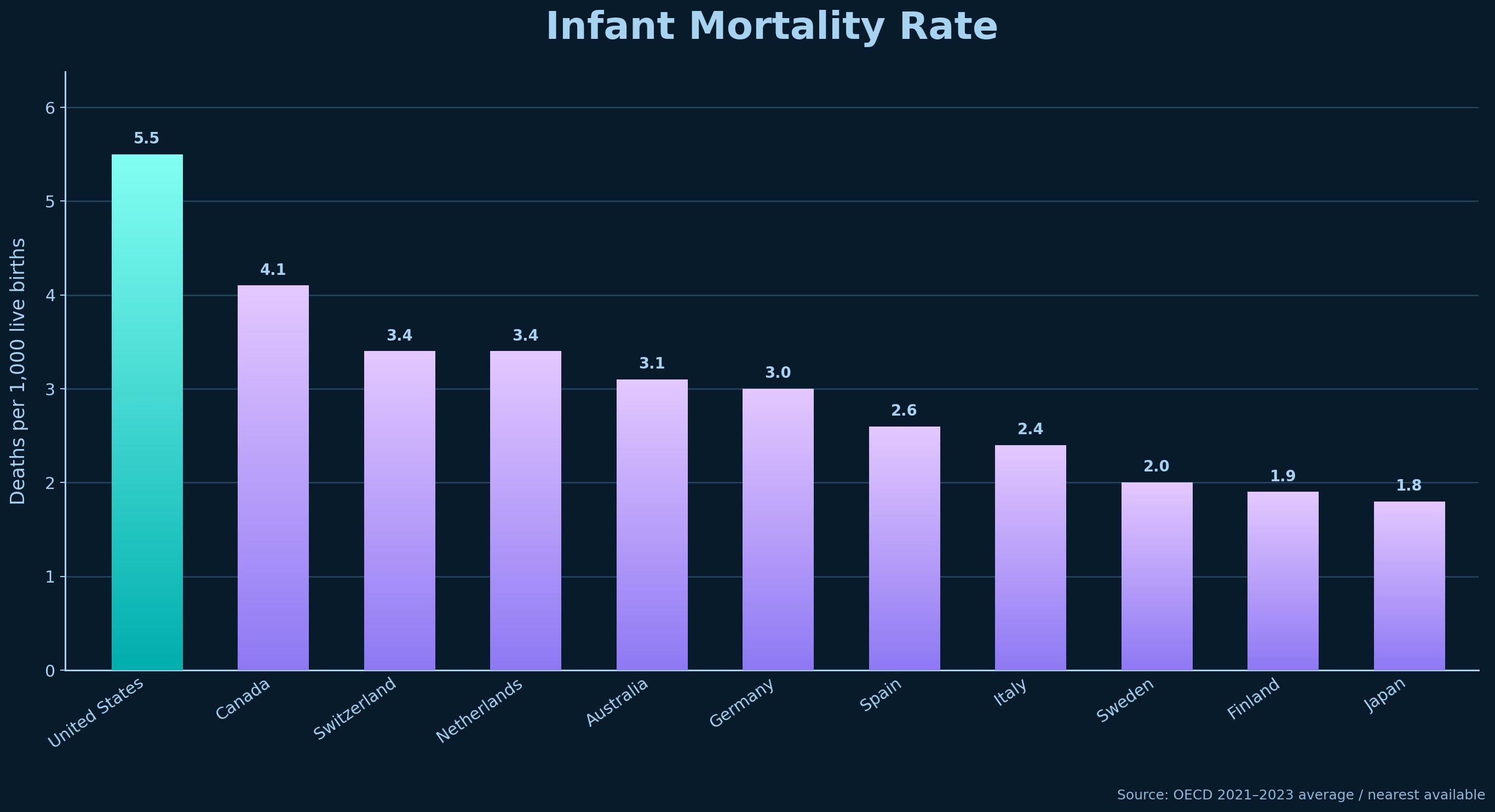
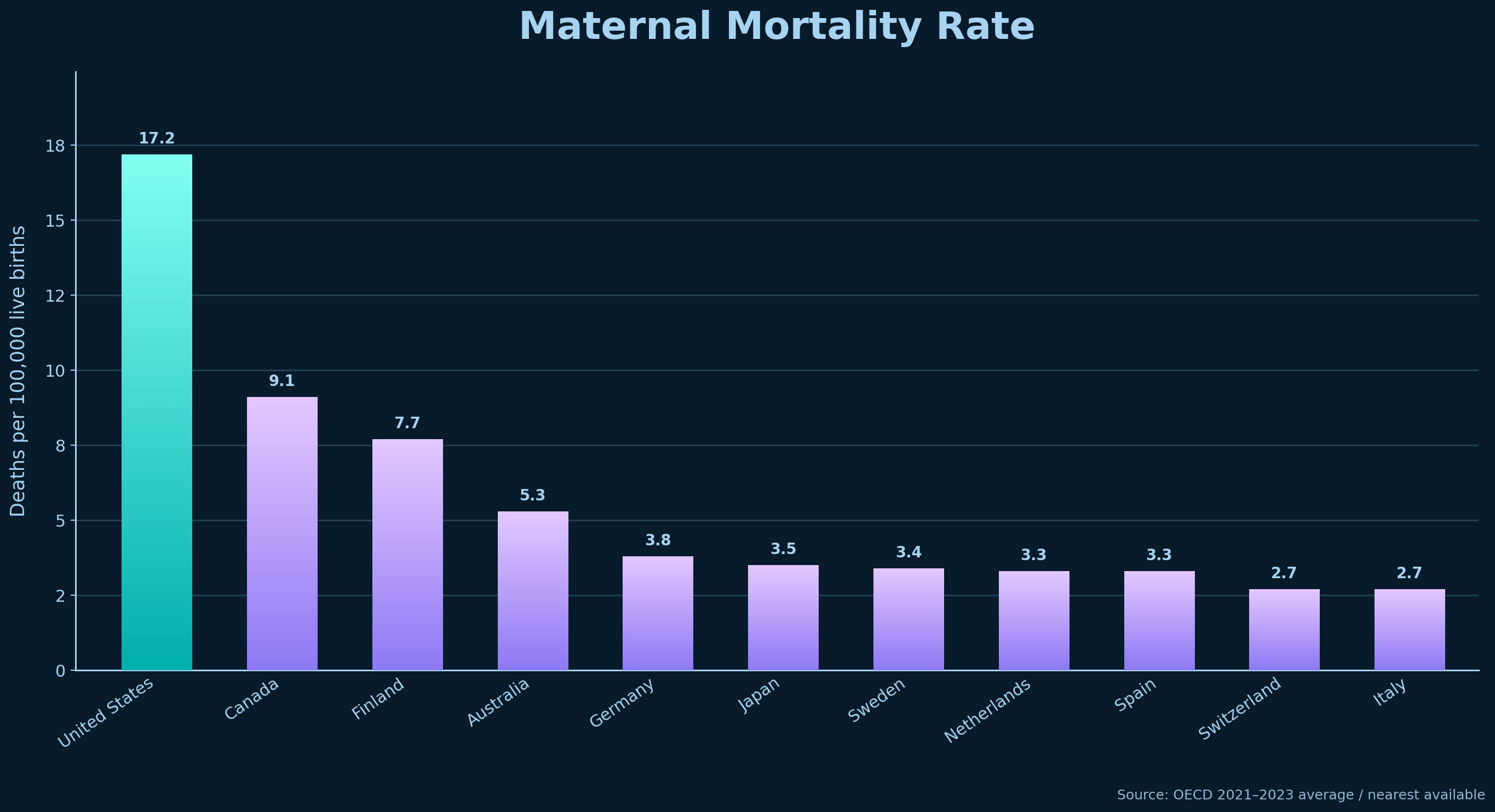
Two other critical metrics are Infant and Maternal mortality rates. Maternal mortality rate is the number of mothers who die due to pregnancy or childbirth-related issues. And the infant mortality rate is the number of children under the age of 1 who die.
Tragically, among peer nations, the United States leads in both of these death rates. The US has a maternal mortality rate of 17.9, compared to some peer nations that are below 3, and an infant mortality rate of 5.61 compared to nations like Japan and Finland that are below 2.
America has a long way to go to become a leader in healthcare.
Sources for this section
OECD Health at a Glance 2025: life expectancy, preventable mortality, and treatable mortality
Commonwealth Fund: U.S. maternal mortality compared with other high-income nations
Other Measures of Healthcare Spending
Positive health outcomes are the primary concern of most people, but there are other ways to view what society is getting for its spending. These include the percentage of the population covered, wait times, the number of practicing doctors, the number of hospital beds, and the availability of equipment such as advanced imaging devices.
One of the core aspects of universal healthcare is that everyone in the country is covered by the healthcare system. In the United States, this is not the case. 27 million Americans are uninsured. Recent political decisions are projected to increase this number by millions over the next few years.
The problem extends beyond the uninsured.
Millions of Americans technically have insurance, but still cannot afford to use it. This is called being underinsured. Commonwealth Fund found that nearly a quarter of insured working-age adults were underinsured in 2024, meaning their deductibles, copays, or out-of-pocket costs were still high enough to make care unaffordable.
That is why medical debt exists at the scale it does. People go to the doctor, use the hospital, get surgery, have a baby, or need medication, and then find out their insurance still leaves them with bills they cannot pay. Only 56% of Americans are fully, properly insured for the full year.
Universal healthcare is not only about handing someone an insurance card. It is about ensuring the card actually protects them from financial disaster when they get sick. America’s system fails people with and without insurance alike.
Our peer nations do better on routine and preventative care. Only two in five US Medicare beneficiaries who needed to see a doctor could book an appointment within 2 days when they were sick. In the Netherlands, 61% can book an appointment on short notice, and 85% can get same-day responses to medical questions.
One reason is that in the US, there are only 2.7 practicing doctors per 1,000 people. In Australia, there are 4.2, and in Germany, 4.7. The US has fewer hospital beds as well, with 2.8 per 1,000 people compared to Germany’s 7.7 and Japan’s 12.5.
There are a couple of bright spots for the US. The average wait time for specialized, elective care is lower than in peer nations, and the US has more CT/MRI/PET units than other nations.
America has built a system that is very good at expensive specialized care, because that is where the money is. A profit-driven system pushes more specialized elective care, which carries higher profit margins and better pay, but at the cost of worse routine and preventive care.
The good news is that there is no need for America to lose its advantage in specialized care as we solve our healthcare problems. We can preserve high-quality specialized care while also making routine care affordable, reducing medical debt, expanding coverage, and catching health problems before they become emergencies.
Sources for this section
Commonwealth Fund: older adults’ access to care across countries
OECD Health at a Glance 2025: doctors, hospital beds, medical technology, and population coverage
CBO/KFF: projected increases in the uninsured from recent policy changes
What Is Universal Healthcare?
There is a common misconception in the United States that universal healthcare means having a single-payer system. Single-payer is one form of universal healthcare, but not the only one. There are multipayer systems, as well as public-private partnerships. At its core, universal healthcare is based on two principles.
Every resident has healthcare
Medical care does not create financial hardship
Let’s look at some different systems to see how they work.
Single-Payer
Single-payer healthcare means that all citizens pay into the same healthcare financing system. In other words, healthcare is publicly funded through taxes and mandatory contributions. But even single-payer healthcare systems are not all the same.
In the United Kingdom, Norway, Denmark, and Sweden, the government, either nationally or regionally, owns many of the hospitals and healthcare facilities and directly employs healthcare workers. It is government-funded and government-operated.
In Canada and Taiwan, the government collects the money for healthcare and then pays out to privately run providers that operate within the bounds of government regulation on services provided and their costs.
In all universal healthcare countries, there are services that fall outside the core healthcare system, such as cosmetic surgery and other elective procedures. Those services operate more like the U.S. system, where providers set their own prices, and people pay directly or use private coverage.
Multipayer
Where single-payer means that everyone is part of the same health insurance system, multipayer means that there is more than one system.
Germany, the Netherlands, and Japan are examples of multipayer healthcare systems.
Germany mandates that all residents have healthcare and uses a system of highly regulated, nonprofit sickness funds funded by payroll contributions from workers and employers (payroll taxes similar to those for Medicare in America). High-income earners can opt out of the system to use private insurance instead.
The Netherlands also requires all residents to purchase healthcare through heavily regulated private insurers, which must accept all applicants and compete for customers. They are required to offer a standard benefits package to all recipients. The government pays subsidies to make insurance more affordable.
In Japan, all residents must enroll in either the Employees’ Health Insurance through their employer or in the National Health Insurance for the self-employed, the unemployed, and students.
Germany typically has lower out-of-pocket costs for routine care. The Netherlands has an annual deductible similar to many American health insurance plans. Japan has a 70/30 rule in which patients pay 30% of the out-of-pocket cost, while insurance covers the remaining 70%. There are adjustments in copay for children and low-income seniors, and there are monthly caps on healthcare costs based on income to prevent financial hardship from severe medical bills.
Universal healthcare does not require one specific model. Canada is different from Germany. Germany is different from Taiwan. Taiwan is different from the Netherlands. The Netherlands is different from Australia. All of those nations are considered among the top 10 for healthcare. Taiwan routinely ranks first and has a satisfaction rate over 90%.
Sources for this section
What Should the United States Do?
For years, polling has consistently shown that the American public believes it is the federal government’s responsibility to ensure that all citizens have health care coverage, while also expressing concern that health care costs are rising too much.
Whether they realize it or not, those responses are asking for universal healthcare. While the top 5 healthcare systems in the world are all single-payer, which is also the most cost-efficient approach to healthcare, America does not appear ready to make that change.
When polls ask specifically about the type of universal healthcare, the public is split. There is as much support for a single-payer system as for a public/private split. That is where we should start, with deciding how to create a system that will guarantee every citizen affordable healthcare while being accepted by the majority of the public as the right path forward.
Interestingly, the original plans for the Affordable Care Act were intended to address this.
This included mandating that all Americans have health insurance, just like the multipayer systems in other nations such as Germany, the Netherlands, and Japan. This was part of the ACA legislation that was passed. It was called the individual mandate. But opponents fiercely attacked the measure, even taking it to court. The end result was that the individual mandate remained technically still part of the ACA, but the penalty for not carrying insurance was reduced to $0, rendering it meaningless.
There are two reasons to mandate that everyone has healthcare.
The first is that it means people have health insurance when they need it. So if they have a serious accident or illness, they receive proper care to get them healthy, rather than relying on emergency room care or going bankrupt from the costs.
The second reason is that having everyone insured lowers insurance costs. Requiring all drivers to have car insurance keeps costs down because most drivers won’t need to file a claim in any given year. Their funds go to those who do have accidents, keeping the program working. The same is true for healthcare. If only those who are currently sick have healthcare, then the cost of healthcare would be extremely high. If all healthy people also carry health insurance, costs stay low. Then, when those healthy people need care in some future year, they’ll have it without having to spend a fortune out of pocket.
Another aspect the ACA originally intended to address was providing people who want government-provided healthcare with a public option, meaning they could get their insurance directly from the government rather than a private insurer. Under this system, private insurance companies would still exist, but the public has a choice between public and private insurance.
The health insurance companies aren’t big fans of the public option because they understand the government will negotiate lower prices, forcing them to lower their costs as well, thereby reducing their profits.
Independent Senator Joe Lieberman killed the ACA public option. His vote was needed to reach the 60 votes in the Senate required to pass the regulation against a Republican filibuster. He refused to vote for the ACA without the public option removed.
Requiring every citizen to have health insurance and offering a public option would be the first step toward a universal healthcare system. The next step would be to establish regulations defining maximum and out-of-pocket costs for various services and treatments, with a heightened focus on routine and preventive services. Treating illnesses earlier reduces the need for expensive treatments, reduces lost workdays, and helps people live longer, healthier lives.
By adding a public option, people get to see how government healthcare works. If they prefer it to the private options, America can take the next step toward a single-payer system and save even more money. If people like what private insurance companies are offering, the US can remain a multipayer system.
We can build an American version of universal healthcare that covers everyone, lowers costs, reduces medical debt, protects routine care, and preserves access to high-quality specialized care.
Sources for this section
Pew Research Center: Americans’ views on government responsibility for health coverage
Gallup: support for government ensuring healthcare coverage and public/private split
AP-NORC: health cost concerns and support for federal responsibility
IRS / Healthcare.gov: individual mandate penalty reduced to $0
Commonwealth Fund / CQ HealthBeat: public option dropped during ACA negotiations
Conclusion
Universal healthcare is used by the rest of the world because guaranteeing that all citizens have affordable comprehensive insurance works. It creates better outcomes and lower costs. America needs to stop treating universal healthcare as a synonym for single-payer healthcare and start implementing solutions that will address our high costs and poor outcomes.
The United States does not have to choose between doing nothing and copying another country’s system. We can guarantee coverage, lower drug prices, cap out-of-pocket costs, reduce medical debt, and invest in routine and preventive care. We can rein in prices while preserving access to high-quality specialized care.
The only thing stopping this progress is the misinformation that makes Americans believe that the most expensive healthcare system in the world, with worse outcomes, is the only one we can afford.
Receipts: Social Security Does Not Add To The National Debt

There is plenty of confusion about how Social Security is budgeted and how its funds have been used in the past, which makes it a target for misinformation from those who want to eliminate or destroy the program.